
Manufacturing Consensus: How “Evidence Generation” Became Policy Laundering in Australia’s Vaping Debate

https://nceph.anu.edu.au/research/research-projects/health-impacts-electronic-cigarettes/national-e-cigarette-monitoring-and-evidence-consortium
National E-cigarette Monitoring and Evidence Consortium
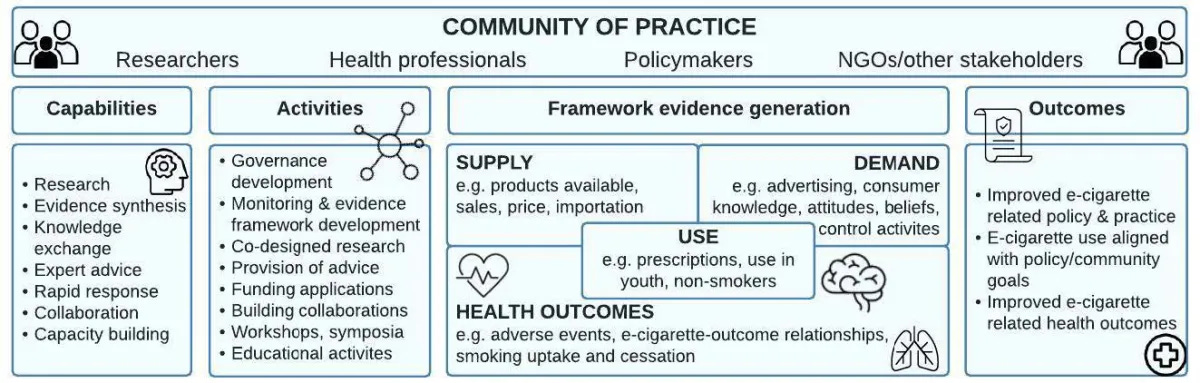
There is a particular style of diagram favoured by modern public health bureaucracies. It is neat, technocratic, and visually reassuring, filled with boxes, arrows, and neutral-sounding language like “frameworks,” “capabilities,” “outcomes,” and “communities of practice.” It presents itself as objective and evidence-driven. Yet beneath that surface neutrality often lies something far more political. The framework used to justify Australia’s e-cigarette policy architecture is a textbook example of policy-driven bias disguised as evidence generation. It does not exist to discover truth or test competing hypotheses. It exists to justify decisions already made.
The most revealing feature of this framework is not what it measures, but where everything leads. Every activity, every capability, every form of “evidence generation” flows toward predetermined outcomes such as “improved e-cigarette policy and practice” and “e-cigarette use aligned with policy and community goals.” Nowhere does the framework point toward uncertainty reduction, falsification, or genuine exploration of whether current policies are working or failing. When desired policy outcomes are embedded at the top of the model, the work beneath them is no longer scientific inquiry. It is a rationalisation.
Equally telling is who the framework centres and who it excludes. The so-called “community of practice” is composed of researchers, health professionals, policymakers, and NGOs. Absent are adult consumers, smokers who quit by switching to vaping, and people managing nicotine dependence in the real world. Use itself is framed almost exclusively as a problem of youth uptake, non-smokers, and inappropriate access, rather than as a harm-reduction pathway for people who would otherwise smoke. This omission is not accidental. Including adult users would complicate the narrative, introduce trade-offs, and force policymakers to confront benefits alongside risks. Ideology is far easier to maintain when lived experience is excluded.
The treatment of demand reveals the same mindset. Advertising, beliefs, attitudes, and knowledge are framed as forces to be controlled rather than understood. There is no recognition that informed adults may rationally choose lower-risk products. Demand is something to suppress, not something to respond to. This reflects a deeply prohibitionist worldview in which people do not exercise agency but are acted upon by influences that must be neutralised. Once this assumption is embedded, paternalism becomes not only acceptable but virtuous.
Health outcomes within the framework are similarly selective. Emphasis is placed on adverse events, vaping-related harms, and smoking uptake, while benefits such as smoking cessation, substitution effects, and reduced exposure to combustion are marginalised or omitted altogether. Entirely missing are counterfactuals: what happens when vaping is restricted or banned, what happens to smoking rates, and what unintended consequences emerge. Outcomes that might contradict the preferred narrative simply do not exist within the model. Evidence is not weighed; it is filtered.
The framework also reveals a closed institutional loop masquerading as collaboration. Researchers, health professionals, policymakers, and NGOs generate evidence, interpret it, advise the government, and then cite each other as validation. There is no adversarial process, no independent challenge, and no mechanism for correction when policies fail in the real world. Rising smoking rates after restrictions are not treated as signals to re-examine assumptions but as communications problems requiring better enforcement or messaging. The system is designed to persist, not to learn.
Perhaps the most revealing phrase in the entire framework is the goal of “aligning e-cigarette use with policy and community goals.” This is not a public health objective. Public health should align policy to evidence and lived outcomes, not force behaviour and evidence to conform to predetermined goals. When alignment replaces inquiry, governance supplants science.
The stated objectives of the consortium that sits behind this framework reinforce the same structural bias. The declared aim is to “improve health by informing policy and practice on e-cigarettes.” Health is not defined independently or measured as an outcome in its own right. Policy success becomes a proxy for health success, even when real-world data contradicts that assumption. This is governance-first public health, where evidence informs policy rather than testing it.
The much-touted “community of practice” is again revealing in its exclusions. Researchers, policymakers, health practitioners, and NGOs are included; adult consumers, ex-smokers, dissenting scientists, harm-reduction experts, and international voices from successful regulatory environments are not. This is not pluralism. It is institutional self-reinforcement. Knowledge exchange occurs only within approved boundaries, among actors who share incentives, funding streams, and ideological commitments.
The consortium emphasises its independence from tobacco and e-cigarette industry influence, yet says nothing about independence from government funding incentives, WHO frameworks, advocacy-driven NGOs, or career and reputational pressures. Removing one source of bias while ignoring all others does not produce objectivity. It merely selects which biases are acceptable. Independence is not just about who writes the cheque; it is about freedom to disagree without penalty.
Claims of identifying “evidence gaps” ring hollow when the framework itself predefines what counts as relevant evidence. Youth uptake, adverse events, and control activities are prioritised, while substitution effects, displacement, black-market dynamics, and smoking relapse after restrictions are excluded. When institutions define the gaps internally, they also define the answers.
Even the language of “capacity building” reveals its purpose. Capacity is not built to challenge assumptions or revise policy in light of failure. It is built to train more people in the same framework, expand surveillance aligned with existing goals, and institutionalise a single interpretation of evidence. This is not scientific progress. It is policy entrenchment.
The membership list of the consortium makes the structural problem unavoidable. It is not a collection of independent experts but a tightly networked institutional bloc dominated by Cancer Councils, Quit organisations, government health departments, and universities embedded in tobacco-control funding ecosystems. These entities co-author research, advise governments, fund one another, and advocate publicly in lockstep. Many of the same individuals help design policy, study its effects, and then return as expert validators, citing each other’s work as consensus. This is circular authority, not independent science.
Advocacy organisations dominate what is presented as evidence generation. Their mission is not to neutrally test whether vaping reduces harm under specific conditions, but to reduce nicotine use and advance restrictive controls. When advocacy bodies control the production and interpretation of evidence, outcomes are effectively pre-decided. Research becomes a tool to defend policy rather than a method to evaluate it.
None of this requires dishonesty or bad faith on the part of the individual. The problem is structural. It is a system in which funding, careers, reputations, and institutional legitimacy depend on alignment with a particular policy worldview. Independence is framed narrowly as the absence of industry ties, while dependence on government and advocacy orthodoxy is normalised and invisible.
When the same institutions that design policy also control the evidence used to justify it, the result is not evidence-based public health. It is a managed consensus. And when evidence is managed rather than tested, the language of science becomes a tool of governance rather than a means of discovering what actually improves health.
It is like money laundering, but instead hides the lives lost… It is criminal, or if it isn’t it should be.
How tragic, sad and warped to be part of this 😢
On a serious level, how much of an influence do bloomberg's “envelopes of death” have on current policies?